- Timeless Autonomy
- Posts
- The LEAD Model and Your Secret Clinical Advantage
The LEAD Model and Your Secret Clinical Advantage
Why CMS' LEAD makes clinician-strategists more valuable than ever. Plus: Breaking down two parts of LEAD with their signals and opportunities
Dana Prommel Strauss
April 05, 2026
Table of Contents

The Long-Term Enhanced ACO Design (LEAD) Model’s long-awaited Request for Applications is out. Applications are due May 17th, and CMMI graciously made the application abbreviated for ACOs already participating in ACO REACH!
My initial thoughts when the basics of LEAD were announced in December of 2025 can be found here.
Since I’m not doing a deep dive summary of LEAD today, here’s a super comprehensive and awesome landing page with organized details about the model made by Brad Heywood. Check out the cards that link out to all the relevant areas! 👏 👇️

Here are two components of LEAD that I’m particularly interested in:
CMS Administered Risk Arrangements
Testing of “AI Inferred Risk”
Let’s dive in:
CMS Administered Risk Arrangements (CARAs)
This model is the first time CMS is testing CARAs. They are a voluntary option for ACOs in Global Risk Arrangements only.
The idea is this:
Some ACOs whose patients overlapped with other CMMI episodic models’ inclusion criteria, like the Bundled Payment for Care Improvement Advanced (BPCI-A) Model, would receive what I called “bundle data” at the time.
From that data, they could (and we did) build longitudinal views of patient journeys. Combine that with access to EMRs along that journey and we were able to identify root causes of avoidable spend and poor patient outcomes and address them. For those patients who overlapped with our ACO patients, the value was actually exponential.
Called out by Premier, Inc. and others, CMMI saw the value in this data and began providing it to ACOs for their attributed patients. So let’s say my patient Mrs. Smith is in my ACO and had a hip fracture with ORIF. If that patient “fell into” a BPCI-A program, that would trigger a “surgical hip and femur fracture treatment” DRG and that would trigger a BPCI-A episode. So CMMI started sharing the same information on that episode with the ACO as if they were also participating in BPCI-A and the patient “fell into” that episode.
Some ACOs have used that data like we did back in the late 20-teens, mapping patient journeys and addressing root causes of potentially avoidable high cost and lower quality care that led to poor outcomes. That information and those insights could be shared with providers in the community along the continuum that provided care to the patient for some portion of time during the episode. It’s a powerful way to help incentivize care transformation!

From the Notioly Collection
Enter the LEAD Model, and CARAs are an embedded part of the model. CMS is offering two options:
Default. ACOs can choose CMS-constructed Episode-Based Cost Measures (EBCMs). They may not be customized for which codes are included or the episode lengths (acute + 30 vs. 90, for example) but can be customized for certain quality measures and discounts. Great starting point.
“Max Flex.” Here’s where it really gets interesting. ACOs can now customize existing EBCMs and can even work with vendors for alternate episode construction! Requires more advanced analytics and experience with episodes. Prior overlap with BPCI-A or the Comprehensive Care for Joint Replacement (CJR) model? Ideal.
It gets even more exciting! 😂
Not only will there be acute medical, surgical and procedural episodes, but CMS will phase in chronic condition episodes! I’m sure I’m not the only one thinking about how beautifully, and likely intentionally, this overlaps with the ACCESS Model.
And enter the Resilience and Independence in a Safe Environment (RISE) to Age in Place falls prevention episode! 🥳 🙌
I spent years working in and then with home health and can’t say enough about how big the opportunity is to improve quality of life, the ability to age in place, and to reduce total cost of care if we can prevent a percentage of falls via addressing balance impairments and home modifications.
CMS establishes Level II HCPCS G-codes for RN and OT services that will be zeroed out. My only beef here is PT should be included. PT at home can be provided under Medicare Part B for medically necessary balance training and other interventions. For my PT friends, it’s a great opportunity to collaborate with your local ACOs on this!
For all the details, find the LEAD RFA here. The resource linked above by Brad Heywood is another great starting point.
Why I Love CARAs:
The overlap of ACOs and Episodes of Care is a powerful one. My past experience taught me the value of managing both total cost of care and embedded episodes of care. Episodes of care, especially the acute care episodes, are often triggered by the most vulnerable of our population.
And it’s a jungle out there!
Transitions of care, competing incentives of post-acute providers, data-sharing challenges, medication reconciliation issues and much more are inherent risks for anyone, but especially our most vulnerable. The outcomes of an episode can influence someone’s life literally forever. There is still so much opportunity to do better. Embedded episodes create an incentive for ACOs to invest in care continuum navigation, post-acute partnerships, strengthening home-based care opportunities, and more.
My biggest fear? ACOs don’t volunteer.
Preferred Providers
I don’t have the data, but ACO REACH entities largely haven’t jumped on the bandwagon to enter into downstream contractual relationships with specialists and other providers like post-acute providers and rehab therapy clinics. Yet we know a high percentage of spend lives right there!
My wish for LEAD: Much greater adoption of Preferred Provider relationships and widespread participation in CARAs.

Testing AI Inferred Risk Adjustment
Risk adjustment in Medicare Advantage and Fee-for-Service value-based care models is the topic of book chapters and out of scope for this article.
Here’s an article by the Commonwealth Fund covering the basic and a visual snippet from the article 👇️
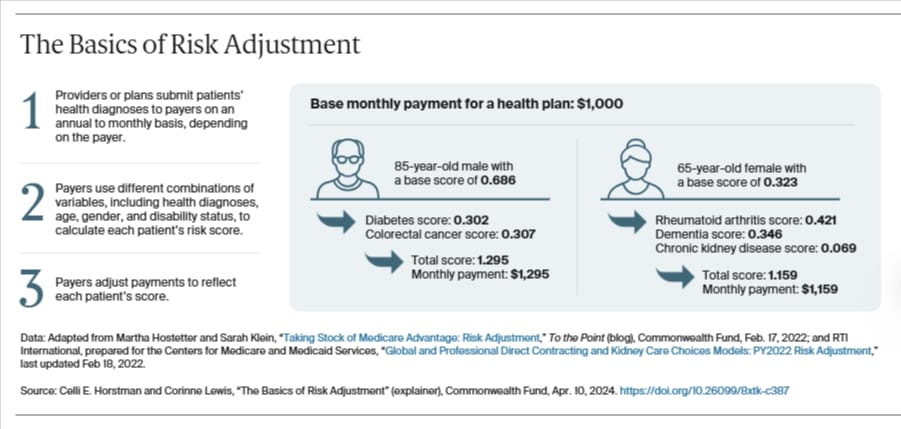
Risk adjustment in Medicare was developed to prevent adverse selection by plans so that CMS pays plans more for beneficiaries with a higher risk of medical spend based on certain diagnoses and demographic information. Diagnoses must be identified by physicians (and advanced practice providers) to determine this component of the risk adjustment factor. ACOs use the same methodology but calculate expected spend a bit differently, and it varies based on the model.
In LEAD, CMMI is actually doing two things with risk adjustment for the first time.
First, they are embedding three different models based on beneficiary category.
Aged and Disabled
End Stage Renal Disease
High Needs (which had its own Track in ACO REACH whose participants were all at-home medical providers like Harmony Cares).
Three different risk adjustment models is exciting in and of itself.
But then, they added a twist.
CMS will test a transition away from provider-identified diagnoses to construct an individual’s risk adjustment factor annually to an artificial intelligence “inferred” risk.
This is not the first time “inferred risk” has come up. Abe Sutton, now Director of the CMS Innovation Center (CMMI), and Gabe Drapos, the COO of Pearl Health, wrote what is now an infamous Health Affairs article in 2024 called “Inferred Risk: Reforming Medicare Risk Scores to Create a Fairer System.”

Here’s how this will work in LEAD:
In 2027 and 2028, CMMI will calculate benchmarks and reconciliation in LEAD using the standard risk adjustment methodology and the LEAD Model specifics.
In 2028, they will “shadow test” AI-Inferred Risk.
In 2029, the AI weight of risk adjustment will be 33%.
In 2030, the AI weight of risk adjustment will be 67%.
And in 2031, risk adjustment in LEAD will be 100% captured by AI inferred risk.
Here’s my take:
CMMI tests new models and methodologies to incentivizing and paying for care in Medicare and Medicaid.
They are testing inferred risk adjustment in the fifth generation of the advanced ACO model at CMMI (Pioneer ACO → Next Gen ACO → Direct Contracting → ACO REACH → LEAD).
They have been refining and adapting the advanced ACO model with each generation. And for the skeptics out there—it’s incredibly hard to change how care is paid for, incentivized, and especially, delivered. Healthcare is unique in many ways. It makes total sense that research and development through model tests have been needed to get us this far.
If inferred risk is successful, keep this in mind next: CMS has always used the same HCC Model for Medicare Advantage and the ACO Models. We saw that most recently in the move from V24 to V28 of HCC, when CMS finalized a three-year phase in of the new model. They created the same phase-in for MSSP and ACO REACH.
So if successful model tests lead to successful permanent models or model components being adapted in Medicare, and if CMS has always used the same risk adjustment model in MA and FFS ACOs, there’s a more than minimal possibility that inferred risk becomes the model used in MA in the future, too.
No doubt there will be refining of the model over the next few years. CMS as the payer in a CMMI model is more able to manage these refinements than plans are. So it makes sense to test first in LEAD.
More to come on the details of the new AI Inferred Risk Model in the future.
Note: Martin Cech also covered this nicely and in more detail in his “Weekly Health Policy Briefing 04/02/2026” post for Health Tech Nerds.
|

Reply